
-
Samadhan Prakashrao Debaje reacted to this post about 4 years ago
India – Strengthening Urban Immunization is Need of Time & action plan to reduce inequities and improve coverage
India is making efforts to increase full immunization coverage by designing various strategies as Special immunization campaigns as Missions Indradhanush due to observed slow growth from past trends.
Though efforts are being done at various level for improvement still there is not equity among various fronts as Urban vs Rural, Poor vs Rich, educated vs Illiterate, states vs Union Territories, and issue of inequities is observed among different platforms.
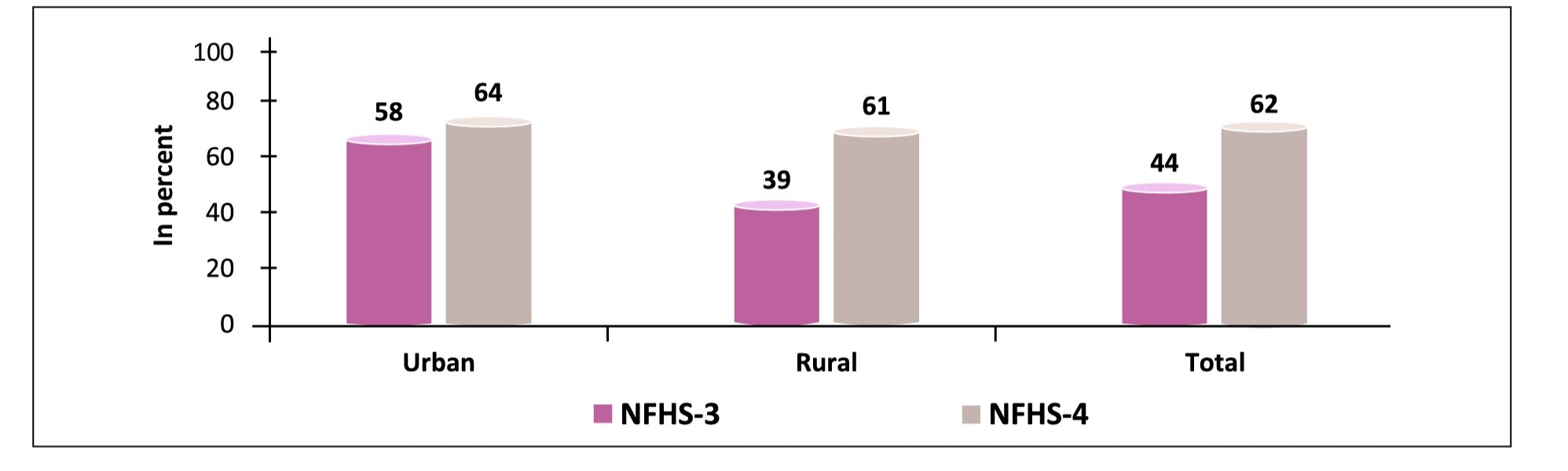
Still mostly one major front always remains neglected i.e. difference rate at which immunization coverage in Urban and Rural areas is improving, this can be seen with the help of figure below. As per UN world urbanization report 2018 India’s 34% population is living in Urban areas, and it will be around 60% by year 2030.
Currently we can see growth in immunization coverage in urban areas compared to Rural is slow as...
MoreIndia – Strengthening Urban Immunization is Need of Time & action plan to reduce inequities and improve coverage
India is making efforts to increase full immunization coverage by designing various strategies as Special immunization campaigns as Missions Indradhanush due to observed slow growth from past trends.
Though efforts are being done at various level for improvement still there is not equity among various fronts as Urban vs Rural, Poor vs Rich, educated vs Illiterate, states vs Union Territories, and issue of inequities is observed among different platforms.
Still mostly one major front always remains neglected i.e. difference rate at which immunization coverage in Urban and Rural areas is improving, this can be seen with the help of figure below. As per UN world urbanization report 2018 India’s 34% population is living in Urban areas, and it will be around 60% by year 2030.
Currently we can see growth in immunization coverage in urban areas compared to Rural is slow as Rural coverage increased from 39% to 61 %(i.e. growth of 22%) whereas Urban coverage growth from 58% to 64%(i.e. 6% only) So now it becomes most important to review current efforts taken to focus more on Urban population as these are not so much helping in current scenario and ways to improve Urban immunization coverage.
In India main Immunization related activities are as same as Rural areas in term of planning and reporting. Though it seems that India is focusing to improve Urban immunization coverage but on reality there are many shortcomings/weakness/barriers in system as below: -
- • NUHM is formed and constituted with budget allocation. In year 2018-2019 the allocation for National Urban Health Mission (NUHM) has increased by 34% at Rs 875 crore BUT The allocation for the funding pool for immunization has decreased by 30%. * (Source: Demand Nos. 42 & 43, Ministry of Health and Family Welfare, Union Budget 2018-19, PRS.)
- • Though allocation of FHW (Female health worker-ANM) post are filled in most of urban areas, there areas demarcation for responsibility allocation in term of immunization activities is uncertain and not as per need, so most of the beneficiaries needs to visit Urban headquarter hospitals for Vaccination services.
- • Though ANM /FHW are there but a crucial link between FHW/ANM and community i.e Accredited Social Health Worker (ASHA), who were appointed for community mobilization and tracking of children at community level is missing in urban areas because of Policy decision (Only some slums were given Urban ASHA/USHA)
- • So as in rural area there is 1 ASHA /1000 Population, for tracking of beneficiaries and their mobilization to vaccination site, Urban areas are lacking. Currently Urban areas have been given 1-4 ASHA for only selected areas, though Population ranges from 25 thousand to 10 Lakh (In some metros around 50 lakhs to 1 Crore).
- • Also, as most of the beneficiaries have to visit Urban /District headquarter hospitals for vaccination so area wise due list is not available with FHW/ANM, and so not able to track dropouts or left outs. No mobilization /sensitization is done in urban areas, beneficiaries are expected to come for vaccination on their own knowledge and judgments.
- • No record of vaccination from private practioners in Most of the urban areas.
- • Focus only given to some major areas where vaccination sites are already planned as per previous years planning, no revisions being done to modify Micro plans for Urban areas form past many years
- • ANM /FHW which are posted in Urban areas are mostly dealing with Communicable disease reporting and other programs there is shortage of workdays for Immunization as in most of the states FHW is dedicated to do only 3-4 Immunization sessions in One month, so most of the areas are labelled as TAGGED with Vaccination sites on Paper for microplanning reporting purpose only to show all areas are covered
- • Also timing and far distant vaccination sites due to poor microplanning continuing from past many years in most of the Urban areas not feasible for beneficiaries to travel for too far vaccination sites is Urban areas, as most of the parents are of working communities i.e 8 am to 5 pm but /and timing of vaccination is 9 am to 2 pm \
- • Though data is available for analysis of coverage and which is clearly showing no much growth in immunization coverage, no concrete plans have been decided as Urban task forces are not being conducted at various levels regularly (National/State/District), and mostly on paper without any string decisions.
- • Regarding campaigns under Mission Indradhanush, as there were NO ASHA’s in Most of the urban areas (Except few Urban Slums Named as USHA) for due listing and tracking of children’s, Mission Indradhanush was not helpful as sessions were not planed as per requirement, so ANM planed sessions at regular session site and timing with having “0” or 1 to 2 regular beneficiaries, so overall DROPOUT and LEFT OUT remains as it was.
Opportunities in current context I would like to suggest as follows
- • Policy changes: - In term of HR/ Manpower/Budget allocation dedicated for Urban Immunization, along with use of DIGITAL tools and apps to track vaccination services in urban areas.
- • Supportive Supervision: - Supervisory network for Immunization to be trained for supportive supervisions with help of standard training modules
- • Monitoring: - Monitoring of activities related to Urban immunization to be done by Partners as WHO /UNICEF etc. and inputs to be shared
- • Evaluation: -Regular Urban task force with active participation from agencies working in Urban areas to be done and should be evaluated for progress at all levels with proper documentations of issues identified and action planed and follow ups.
Mode of conducting these activities and reason for selection can be discussed as follows: -
- Identification of beneficiaries ‘and due listing- In Urban context through LQAS in identified States and Urban areas based on available recent coverage evaluation surveys as NHFS, RCM etc. and with use of due listing and mapping through digital tools (Mobile Apps/maps etc.)
- Policy change – Advocacy through Urban Task forces regularly at all levels with its tracking specially for advocating need for special community mobilisers in Urban areas same as of Rural (Accredited Social Health Activist ASHA/ Urban ASHA)-Same can be done with help of identified man powers of other Urban NGO’s and ICDS (Integrated Child Development services) Departments workers i.e. AWW- Anganwadi workers0 also to support communication and mobilization for RI sessions. Also, policy changes for HR recruitment and sufficient budgeting to make accordingly.
- Planning and implementation of Special Vaccination Campaign /activity yearly for selected Urban areas (In 14 states and 7 Metro Urban areas having population over 1 crore) for Due listing, communication and Mobilization of beneficiaries’ (I would like to name it -CMCI Communication and mobilization campaign for Immunization -More details can be obtained from https://www.msjonline.org/index.php/ijrms/article/view/2269 )
- Supportive supervision by in charge Government officers at various level with quality monitoring by Partners as WHO, UNICEF etc. and using surveillance data available and monitoring findings to improve quality of activities undergoing
Post is under moderationStream item published successfully. Item will now be visible on your stream.
Pinned Items
Recent Activities
There are no activities here yet